
Dental implants are one of the most reliable tooth replacement options in modern dentistry. But like any surgical procedure, they carry risks. Understanding these is key to preparing for surgery and making the right decision.
This guide covers everything you need to know about dental implant risks: the real complication rates, the factors that increase your personal risk, and the practical steps that make an unsuccessful outcome far more unlikely.
Are Dental Implants Safe?
The average failure rate for dental implants is approximately 3.1% worldwide. Impressions Dental That figure puts the global success rate above 96%. So yes — dental implants are safe when performed by a qualified specialist on a suitable patient. Decades of clinical research support their use, and millions of implants are placed successfully every year worldwide.
That said, as with any surgical intervention, complications can occur. So let’s take a look at what they are, how common they really are, and what you can do to minimise them.
What Are the Most Common Dental Implant Risks?
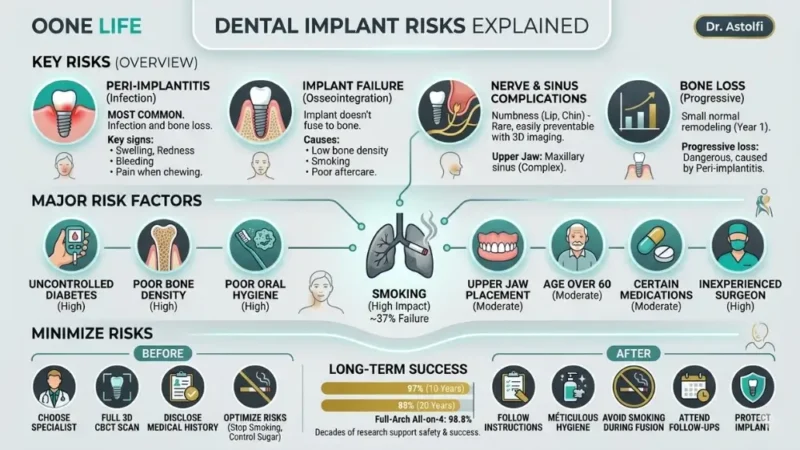
Most complications from dental implants fall into a small number of well-documented categories. Here is what the clinical literature actually identifies:
Infection and Peri-implantitis
Peri-implantitis is the most frequently complication in implant dentistry. It is essentially gum disease around an implant — a bacterial infection that causes inflammation of the soft tissue and, if left untreated, progressive bone loss around the implant.
Research confirms that early failure risk declines significantly after the first year PubMed Central, meaning the post-surgical window is the most critical.
Key signs to watch for:
- Swelling, redness or bleeding around the implant
- Pain or discomfort when chewing
- A bad taste or smell that doesn’t go away
- Visible recession of gum tissue around the implant
Implant Failure and Osseointegration Problems
Osseointegration is the biological process by which the titanium implant fuses with your jawbone. When this process fails the implant becomes unstable and must be removed.
Osseointegration problems are more likely when:
- Bone density or volume is insufficient
- The patient smokes heavily
- Post-operative care instructions are not followed
- The implant is placed in the upper jaw (maxilla), where bone is naturally less dense
Nerve Damage and Sinus Complications
It is worth noting that permanent nerve damage is rare and easily preventable with proper 3D imaging pre-op. However, if an implant is positioned too close to the inferior alveolar nerve, the patient may experience numbness, tingling, or altered sensation in the lip, chin or tongue. In the vast majority of cases, this is temporary.
For upper jaw implants, the maxillary sinus can be affected. Pre-implant sinus lift surgery was identified as a significant risk factor in clinical studies, accounting for 42% of failures in one cohort. Jomos This does not mean sinus lifts should be avoided — it means they require a specialist with specific experience in complex reconstructions.
Bone Loss Around the Implant
A small amount of bone remodeling is considered normal in the first year. What is not normal is progressive bone loss, which can destabilise the implant over time.
A 2024 systematic review found that marginal bone loss across implant studies averaged approximately 1% PubMed Central — a modest figure. Progressive bone loss beyond that threshold is typically associated with untreated peri-implantitis or mechanical overload from a poorly fitted crown.
What Factors Increase the Risks of Dental Implants?

Research has identified patient-related and procedure-related factors that increase the likelihood of dental implant risks, with the 2 main ones being:
Smoking is the single most impactful controllable risk factor. A 10-year retrospective study found that smoking was associated with 37% of implant failures. Nicotine reduces blood flow to the gums and bone, slows healing, and significantly increases infection risk. Quitting — or at minimum reducing — before surgery makes a material difference to your outcome.
Uncontrolled diabetes affects the body’s ability to heal and fight infection. Importantly, well-controlled diabetes does not automatically disqualify a patient — but blood sugar must be optimised before and after surgery in close coordination with your doctor.
Other well-documented risk factors include:
- Poor bone density or volume — insufficient bone cannot adequately anchor the implant post; bone grafting may be required first
- Poor oral hygiene— bacteria accumulate rapidly around implant sites; patients who struggle to maintain hygiene are at higher risk of peri-implantitis
- Certain medications— bisphosphonates (used for osteoporosis), immunosuppressants and some blood thinners can impair healing or increase bleeding risk
- Age over 60— research from UCLA found that increasing age was strongly associated with the risk of implant failure, though age alone is never an absolute contraindication
- Implant location— upper jaw implants fail more often than lower jaw implants; one study found that 83% of failed implants were located in the maxilla, Bite Club where bone is naturally less dense
- Inexperienced surgeon— operator skill is one of the most underestimated variables; complication rates are significantly lower when treatment is performed by a specialist in oral surgery or implantology, not a general dentist
The table below summarises the main risk factors and their relative impact:
Risk Factor | Impact on Failure Risk |
Smoking | High — linked to ~37% of failures |
Uncontrolled diabetes | High |
Poor bone density | High |
Poor oral hygiene | High |
Upper jaw placement | Moderate |
Age over 60 | Moderate |
Certain medications | Moderate |
Inexperienced surgeon | High |
Dental Implant Risk vs. Success Rate
Dental implants are one of the best-evidenced tooth replacement options available with 97% success rate at 10 years. The risks are real but manageable — and for the large majority of suitable candidates, the long-term outcome is excellent.
The long-term picture is equally compelling. At 20-year dental implants showed a survival rate of 88% according to a 2024 meta-analysis covering +1,600 implants, reflecting 4 out of 5 implants succeed after over two decades.
For full-arch solutions show even better numbers. The survival rate of All-on-4 dental implants stands at 98.8% Impressions Dental.
What do these numbers mean in practice? A few key takeaways:
- Most failures are early.Once the initial post-operative period is overcome, implants become significantly more stable, with failure rates declining sharply after the first year. If your implant integrates successfully in the first 3–6 months, the probability of long-term success is very high.
- Failure is not the end.In most cases, a failed implant can be removed, the site allowed to heal, and a new implant placed successfully. It is a setback, not a permanent outcome.
- Success is not passive.The data reflects patients who attended follow-up appointments, maintained oral hygiene, and worked with experienced clinicians. Outcomes deteriorate when any of those elements are missing.
How to Minimise Dental Tooth Implant Risks
The good news is that most dental implant risks are directly influenced by choices you make before, during and after treatment. Here is what the evidence supports.
Before surgery:
- Choose a specialist, not a generalist.This is the single highest-impact decision you can make. Look for a surgeon with specific training in oral surgery, implantology or periodontology. Ask directly: how many implants do you place per year? What is your personal complication rate?
- Get a full 3D scan (CBCT).A cone beam CT scan gives your surgeon a precise map of your bone volume, density and the exact position of nerves and sinuses. Any clinic that skips this step is cutting corners.
- Disclose your full medical history.Medications, systemic conditions, smoking status and previous jaw surgery all affect planning. Nothing should be omitted.
- Optimise controllable risk factors.If you smoke, reduce or quit at least 2–4 weeks before surgery. If you have diabetes, work with your GP to stabilise your blood sugar. If you are on bisphosphonates, discuss timing with your prescribing doctor.
After surgery:
- Follow post-operative instructions precisely.Antibiotics and anti-inflammatories are prescribed for a reason. Take the full course.
- Maintain meticulous oral hygiene.Soft brushing around the implant site, antibacterial mouthwash and interdental cleaning are non-negotiable during healing.
- Avoid smoking during osseointegration.The 3–6 month healing window is the most critical period. Smoking during this phase dramatically increases failure risk.
- Attend every follow-up appointment.Early signs of peri-implantitis or poor integration are manageable when caught early — and irreversible when ignored.
- Protect the implant from excessive force.Avoid hard foods in the early weeks. If you grind your teeth at night, tell your clinician — a night guard may be recommended.
Why Would a Dentist Not Recommend an Implant?
A responsible dentist will not recommend an implant if the risks outweigh the benefits. This is not a reason to panic — it is good clinical practice.
The most frequent contraindications include:
- Insufficient bone volume.If the jawbone has deteriorated significantly — due to tooth loss, gum disease or prolonged denture use — there may not be enough structure to anchor an implant safely. In many cases, bone grafting can resolve this, but it adds time and complexity to treatment.
- Uncontrolled systemic disease.Active, poorly managed diabetes, autoimmune conditions or recent cancer treatment (particularly head and neck radiation) can severely impair healing. The implant may not be ruled out permanently — but treatment must wait until the condition is stabilised.
- Active gum disease or infection.Placing an implant into an infected or inflamed site is a predictable path to failure. Any existing periodontal disease must be fully treated and resolved before implant surgery begins.
- Heavy, uncontrolled smoking.Some clinicians will decline to place implants in patients who smoke heavily and are unwilling to reduce, given the significantly elevated failure risk.
- Certain medications.Bisphosphonates — prescribed for osteoporosis — can interfere with bone healing and increase the risk of a rare but serious condition called osteonecrosis of the jaw. This does not automatically rule out implants, but requires careful specialist assessment.
- Insufficient patient commitment.Implant success depends on long-term maintenance. A patient who is unlikely to maintain adequate oral hygiene or attend follow-up appointments may be better served by an alternative solution.
Are Dental Implants Worth the Risk?
For most suitable candidates, yes — dental implants are worth it. But it is always a personal calculation that depends on your health profile, your expectations and the quality of care you receive.
Here is how to think about it honestly.
What you gain:
- A permanent, fixed solution that looks, feels and functions like a natural tooth
- Prevention of bone loss— unlike dentures or bridges, implants stimulate the jawbone and prevent the gradual deterioration that follows tooth loss
- No impact on adjacent healthy teeth — unlike a traditional bridge, which requires grinding down neighbouring teeth
- Long-term cost efficiency — a well-maintained implant can last decades, making it cheaper over a lifetime than repeated denture repairs or replacements
- A measurable improvement in confidence, comfort and quality of life — consistently reported in patient satisfaction studies
What you accept:
- A surgical procedure with a small but real risk of complications
- A healing period of 3–6 months before the final restoration
- An upfront cost that is higher than alternatives
- A long-term maintenance commitment
What Is the Most Painful Part of Getting a Dental Implant?
Fear of pain is one of the most common reasons people delay implant treatment — and in the majority of cases, that fear turns out to be disproportionate to the reality.
Here is what actually happens at each stage.
During the surgery itself: The mouth is numbed with local anaesthesia. You will feel no pain whatsoever. Most patients are surprised by how comfortable the procedure. Sedation options are also available at many clinics for patients with dental anxiety.
In the 24–72 hours after surgery: This is typically the most uncomfortable period and pain is managed with medication. As the anaesthesia wears off, you can expect:
- Mild to moderate soreness around the implant site
- Some swelling of the gum and surrounding tissue
- Occasional bruising, particularly after bone grafting
- A dull ache that responds well to standard over-the-counter painkillers
Are the Risks of Dental Implants in Turkey Higher?
No — not if you choose the right clinic. The risks of dental implants in Turkey are not higher than in the UK or US. What determines your risk is the quality of the surgeon, the technology used, the implant brand, and the standard of aftercare.
Where the real risk lies:
- No 3D imaging before treatment planning
- Vague or non-existent guarantees on the implant work
- A general dentist performing complex implant surgery
- No clear aftercare
- Pressure to decide quickly or pay in full upfront
What to look for in a Turkish implant clinic:
- Surgeons with specialist qualifications in oral surgery or implantology
- Premium, internationally certified implant brands
- Full CBCT scanning as a standard part of the diagnostic process
- Written guarantees and a structured aftercare plan
- Verified independent reviews on platforms such as Trustpilot or Google