Half of adults have some form of gum disease, but most don’t know it. Early signs can be as easy to dismiss as bleeding gums, which is a common symptom of gingivitis. That’s still early-stage gum inflammation: reversible, manageable, and easy to treat. Periodontitis is what happens when gingivitis is left untreated: a condition that eats away at the bone supporting your teeth, and raises your risk of heart disease and diabetes. The difference between gingivitis vs periodontitis could mean a clean or a surgeon. But to the untrained eye, they look almost identical. This is what makes them dangerous.
What is Gingivitis & What Does it Look Like?

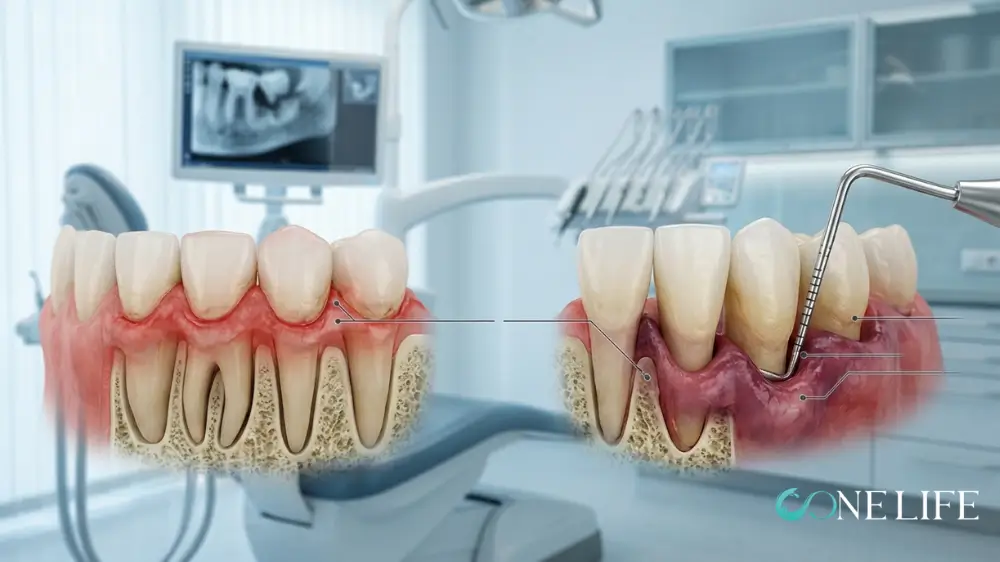
Gingivitis is an inflammation of the gum tissue caused by plaque accumulated at the gumline. The buildup of bacteria triggers an immune response, your gums become irritated, swollen, and fragile. Crucially, at this stage no bone has been lost. This means gingivitis is reversible.
Signs & Symptoms of Gingivitis
- Bleeding gums
- Red or purplish gums
- Swollen or puffy gums
- Persistent bad breath(halitosis)
- Tender gums
- Shiny gum surface
What is Stage 1 Periodontitis & What Does it Look Like?

Periodontitis begins where gingivitis ends but looks almost identical. At Stage 1, pockets are around 4 mm, bone loss of 1–2 mm, and bleeding happens on probing. Once bacteria penetrate below the gumline, the gums begin to pull away from the teeth, forming periodontal pockets which trap bacteria, accelerate infection, and deepen over time. Unlike gingivitis, the bone loss that occurs in periodontitis is permanent.
Signs & Symptoms of Stage 1 Periodontitis
- Gums that bleed on probing
- Periodontal pockets of 4 mm or deeper
- Early bone loss visible on X-ray
- Gum recession beginning
- Persistent bad breath
- Occasional gum sensitivity
- No significant pain
What Causes Gingivitis? In Detail
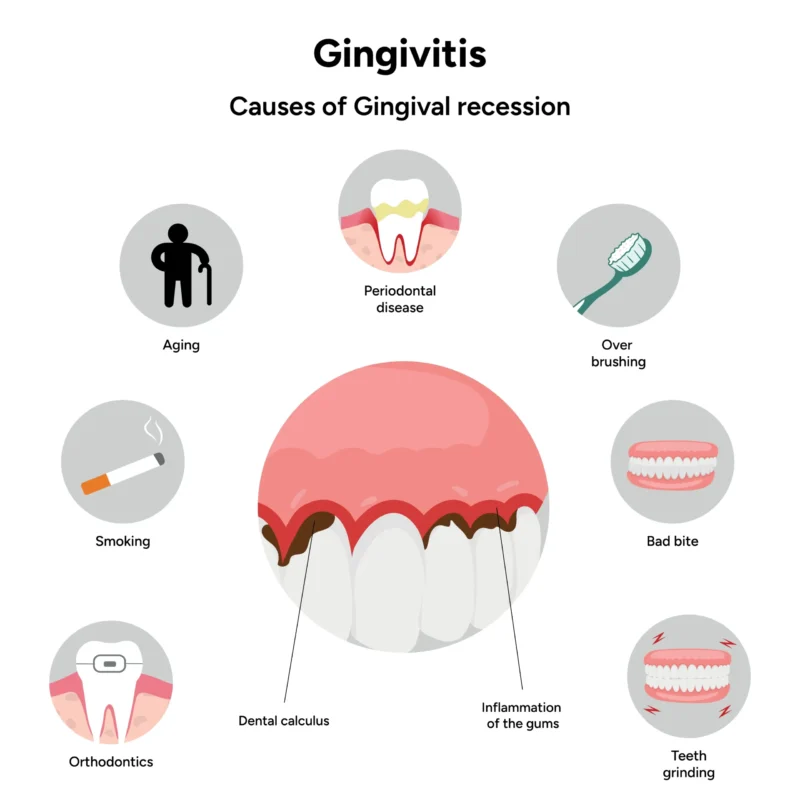
Gingivitis is the earliest stage of gum disease. The most frequent cause is poor or irregular tooth brushing, which allows plaque to remain on teeth. Plaque hardens into tartar (also called calculus) within 24–72 hours and it cannot be removed by brushing alone. Once tartar forms, professional cleaning is the only way to remove it.
Factors That Accelerate Gingivitis
Not everyone with imperfect oral hygiene develops gingivitis at the same rate. Factors that tip the balance include:
- Smoking and tobacco use
- Diabetes
- Hormonal changes
- Certain medications
- Stress
- Poor nutrition
- Crooked or crowded teeth
- Genetic predisposition
Which Stage Are You At?
If you’re trying to work out which stage you might be in, this is your reference point. Before read any further, bear in mind these most important points:
- Pain is a poor warning signal. Both gingivitis and early periodontitis are almost entirely painless. By the time something hurts, the disease is usually well advanced.
- The reversibility window is short. Once you cross from gingivitis into periodontitis — even Stage 1 — the bone loss is permanent. The treatment goal shifts from reversal to stabilisation.
- Pocket depth is the number that matters most. Your dentist measures this at every check-up with a small probe. Anything above 3 mm warrants attention. Above 5 mm is a clinical red flag.
Gingivitis | Stage 1–2 Periodontitis | Stage 3–4 Periodontitis | |
Tissue affected | Gums only | Gums + early bone loss | Gums + bone + tissue |
Bone loss | None | 1–4 mm | 4 mm+ / severe |
Pocket depth | 1–3 mm (normal) | 4–5 mm | 6 mm+ |
Reversible? | Yes, fully | No — but stabilisable | No — requires surgery |
Pain | Rarely | Rarely | Sometimes — abscesses possible |
Bleeding gums | Yes | Yes | Yes |
Bad breath | Mild | Moderate to persistent | Persistent, often severe |
Tooth mobility | None | None to mild | Moderate to severe |
Tooth loss risk | None | Low to moderate | High |
Treatment | Professional clean + hygiene | Deep cleaning (scaling & root planing) | Surgery, grafts, or extraction |
Urgency | Act soon | Act now | Act immediately |
Over 1 Billion Cases of Gum Disease in The World
Gum disease is the seventh most prevalent disease worldwide, with 1.09 billion cases recorded in 2019. Globally, estimates suggest that 20% to 50% of the adult population have some degree of gum disease. In the US, it’s over 40% of adults aged 30 or older, rising to 60% of Americans aged 65 and over. In the UK, approximately 50% of adults have some form of irreversible periodontitis. Frontiers
The economic consequences are enormous: severe periodontitis results in an estimated annual productivity loss of up to $54 billion globally, with direct treatment costs reaching $3.49 billion in the United States and €2.52 billion in Europe.
The 4 Stages of Gum Disease
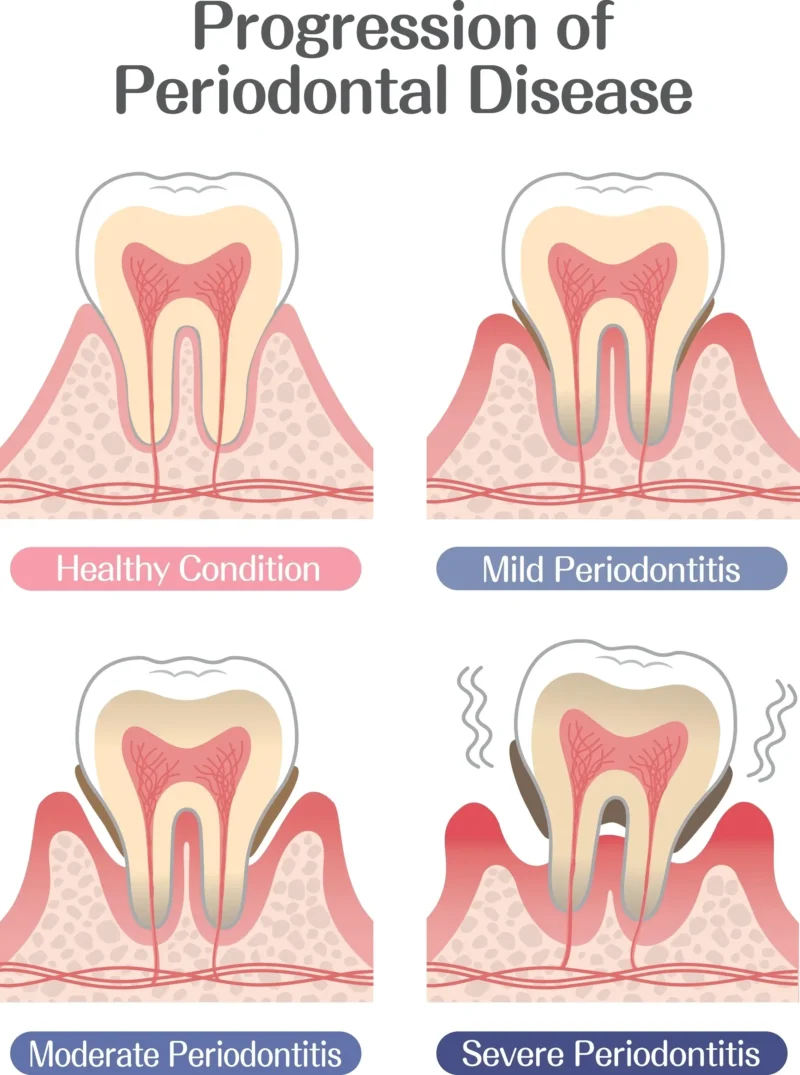
Gum disease doesn’t happen overnight. It progresses through four stages established by the 2018 World Workshop on Periodontal Classification (AAP/EFP). Understanding which stage you’re in determines whether your treatment costs $80 or $8,000, to whether your teeth can be saved at all.
Stage 1 — Initial Periodontitis
Stage I is the earliest form of periodontitis and often develops from untreated gingivitis. It involves mild attachment loss and early bone changes visible on dental X-rays. At this stage, damage is still limited. With professional cleaning and improved home care, progression can often be slowed or stopped.
- Clinical attachment loss: 1–2 mm
- Pocket depth: up to 4 mm
- Bone loss:early, confined to the upper third of the root
- Tooth loss from periodontitis: none
- Reversible? No — but fully stabilisable
Stage 2: Moderate Periodontitis
Stage II reflects increased tissue destruction and disease progression. Gum recession becomes visible. Teeth begin to look longer. Bad breath becomes harder to control. Loss reaches 3–4 mm. Non-surgical treatment is still effective at this stage, but it requires more sessions and more rigorous maintenance.
- Clinical attachment loss: 3–4 mm
- Pocket depth: up to 5 mm
- Bone loss: moderate, still in the upper third of the root
- Tooth loss from periodontitis: none yet
- Reversible? No — requires active professional management
Stage 3: Severe Periodontitis
Stage III involves severe periodontitis with radiographic bone loss extending to the middle third of the root and clinical attachment loss of 5 mm or more, with potential loss of up to four teeth due to periodontal causes. Surgical options — including flap surgery, bone grafts, and gum grafts — become necessary.
- Clinical attachment loss: 5 mm or more
- Pocket depth: 6 mm or deeper
- Bone loss: extends to the middle third of the root or beyond
- Tooth loss from periodontitis: up to 4 teeth
- Reversible? No — surgical intervention often required
Stage 4: Advanced Periodontitis
Stage IV involves advanced periodontitis with radiographic bone loss extending to the apical third of the root, clinical attachment loss of 5 mm or more, with risk of losing five or more teeth and severe masticatory dysfunction. Treatment at this stage is complex, expensive, and prolonged.
- Clinical attachment loss: 5 mm or more
- Pocket depth: 6 mm or deeper
- Bone loss: extends to the lower third of the root or beyond
- Tooth loss from periodontitis: 5 or more teeth at risk
- Reversible? No — complex surgical reconstruction or extraction
What is the Worst-Case Scenario?
Stage 4 periodontitis is a full systemic crisis that starts in the mouth and radiates outward — into your jaw, your confidence, your diet, your cardiovascular system, and your face. The bone supporting the teeth has been destroyed to the lower third or beyond. Pocket depths exceed 6 mm, so that no standard cleaning can reach the bacteria. As the supporting bone disappears, teeth become unsalvageable and may fall out or require extraction. This leads to what’s known as a collapse of the bite. Teeth shift and tilt, jaw alignment changes, and the lower part of your face begins tosink.
The symptoms at Stage 4 include:
- Severe, persistent bad breath
- Visibly receding gums
- Loose and shifting teeth
- Pain when chewing
- Pus between the teeth and gums
- Spontaneous bleeding
- Tooth loss
How to Treat Gingivitis vs. Periodontitis
The earlier you intervene to treat gum disease, the simpler, less invasive, and less expensive your options. There are several treatments depending on the stage you’re in. What your dentist recommends will be influenced by the depth of your pockets, the extent of bone loss, and your medical history. Always try to get a second opinion to evaluate your options.
Here is what treatment looks like at each stage.
Preventive & Early Treatment (Stages 0–1)
At Stage 0 (healthy gums) and Stage 1 (gingivitis), the goal is to remove the bacterial trigger, correct the habits that allowed it to build up, and monitor. When caught early, before any bone loss occurs, proper cleaning and improved oral hygiene can return your gums to perfect health within weeks.
For gingivitis, this means:
- Professional scale and polish: your hygienist removes plaque and tartar from tooth surfaces and just below the gumline using ultrasonic instruments. A standard appointment lasts 30–60 minutes.
- Oral hygiene instruction: brushing technique, interdental brush use, and flossing
- Follow-up assessment at 4–6 weeks
- Cost in the US: $50–$75.
- Cost in the UK: NHS care offers the most affordable option at £27.90–£76.60 in England. Private hygiene appointments typically range from £60–£150
Non-Surgical Treatment (Stages 1–3)
Once periodontitis is established the treatment goal shifts from reversal to stabilisation. The primary tool is scaling and root planing (SRP), also called deep cleaning. It removes tartar and bacteria around the roots of your teeth. It can help bleeding gums and prevent tooth loss.
For moderate to severe cases, localised antibiotics (placed directly into pockets) or antimicrobial rinses may be prescribed alongside SRP to target bacterial load more aggressively.
Here is what the process involves:
- Local anaesthetic is administered
- The dentist or hygienist cleans below the gumline using hand instruments and ultrasonic scalers
- Root surfaces are smoothed (planed) to eliminate rough areas where bacteria collect and to help gum tissue reattach
- Treatment is done by quadrant — typically 2–4 appointments, each lasting 60–90 minutes
- A reassessment appointment follows at 6–8 weeks
- Cost in the US: $400–$4,000 depending on the severity of the disease.
- Cost in the UK: A full mouth course runs £800–£1,600 at private rates, or £76.60 under NHS Band 2 in England.
Surgical Intervention (Stages 3–4)
Periodontitis, once established, is a chronic condition. It can be controlled, but it cannot be cured. Periodontal surgery becomes absolutely necessary when deep pockets cannot be accessed or when bone atrophy is too advanced. Following any surgical treatment, patients enter a lifelong maintenance programme — professional cleanings every 3 months, rigorous home care, and regular monitoring.
Surgical options include:
- Flap surgery (open flap debridement)
- Bone grafting
- Gum grafting
- Guided tissue regeneration (GTR)
How Much Does Periodontal Treatment Cost?
A £199 deep cleaning at Stage 1 becomes £4,000+ surgical treatment at Stage 4. The gap between those numbers represents years of avoided dental visits and normalised warning signs. In the US, full-mouth surgical reconstruction at Stage 4 routinely exceeds $15,000–$40,000.
Systemic Conditions Influenced by Periodontal Disease
The frontier of periodontal research has shifted significantly in the last five years, recognizing periodontitis as a systemic inflammatory driver. A growing body of peer-reviewed evidence — including research published in the British Dental Journal, The Lancet, and Frontiers in Oral Health — now links periodontitis to serious systemic conditions. Dr. Astolfi has actively pursued research on the topic during his scholarship at Columbia University, lecturing at Harvard University.
Heart disease and stroke
The link between periodontal infection and cardiovascular events is now well established in the literature. Research published in the British Dental Journal (2025) confirmed increased cardiovascular risk in people with type 2 diabetes and periodontitis, with outcomes including myocardial infarction, stroke, atrial fibrillation, and dementia.
Cognitive decline and Alzheimer’s
This is perhaps the most alarming emerging area. A 15-year prospective cohort study published in 2026 directly examined the relationship between periodontitis and cognitive decline in older adults, finding a measurable association between chronic periodontal infection and incident dementia.
Diabetes
The connection between periodontitis and type 2 diabetes is bidirectional and now clinically actionable. Diabetes worsens gum disease — and gum disease worsens glycaemic control.
Pregnancy Complications
Research consistently links untreated periodontitis in pregnant women to elevated risk of preterm birth, low birth weight, and pre-eclampsia.
Latest Advancements Periodontal Treatment (2026)
The WHO’s Global Oral Health Action Plan 2023–2030 explicitly identifies periodontal disease as a public health priority. This is one of the most exciting frontiers in modern dentistry right now. The field is moving fast from smarter diagnostics to treatments that regenerate what was considered permanently lost.
AI-Assisted Diagnosis: Catching Disease Earlier
Systems trained on thousands of radiographs can now detect bone loss patterns that a human eye might miss at early stages — potentially catching Stage 1 periodontitis before it becomes Stage 2.
Laser Therapy: Less Cutting, Faster Healing
Laser-assisted periodontal therapy — such as LANAP (Laser-Assisted New Attachment Procedure) — selectively removes diseased tissue while sparing healthy gum, with patients benefiting from less pain, minimal bleeding, and faster healing. A separate technique, antimicrobial photodynamic therapy (aPDT), uses light-activated compounds to destroy harmful bacteria within periodontal pockets without cutting or antibiotics.
Host Modulation Therapy
One of the most important conceptual shifts in periodontology is the recognition that it’s not just the bacteria causing the damage — it’s the body’s inflammatory response to those bacteria. Host modulation therapy (HMT) targets this response directly. Newer agents in development include complement inhibitors and stem cell-derived therapies, with research demonstrating that human periodontal stem cells can modulate inflammatory responses.
Regenerative Medicine: Growing Back What Was Lost
Bone loss from periodontitis has long been considered permanent. That assumption is being challenged. Platelet-Rich Fibrin (PRF) — derived from the patient’s own blood — releases growth factors that accelerate bone and tissue healing when placed into periodontal defects.
Further ahead, 3D bioprinting is emerging as a potential tool for reconstructing the complex multi-tissue architecture of the periodontium — gum, bone, periodontal ligament, and cementum simultaneously.
Gingivitis vs. Periodontitis: A Critical Summary
If you’ve read this far, you now know more about gum disease than the majority of adults who have it. Gingivitis and periodontitis are two stages of the same disease. The bacteria are the same. The trigger is the same.
The critical facts to hold onto:
- Gingivitis is reversible.
- Periodontitis is not reversible.
- Pain is not a reliable warning signal.
- The staging system matters.
- Systemic health is involved.
- The treatment window is real — but finite.